
Propagandizing a Pandemic: The narrative of “progress” in Ghana’s COVID19 response
/It’s been almost a year since Ghana recorded its first COVID19 cases and the situation seems to have gotten worse. On Feb 18, 2021, Ghana’s total case count was 80, 253 with 577 recorded deaths. To be clear, many public health advocates contend that our case count remains a crude underestimate while our hospitals are at capacity treating more severely ill people. Before we recorded our first cases in March, 2020, a number of public health folks warned that COVID19 would strain our fragile health care system even if the burden in terms of numbers were lower than those recorded in Western countries. However, the government boldly declared “We are prepared” without really sharing a detailed public health strategy with the public. This mantra presaged how their propaganda machine would attempt to construct and maintain a façade of effective COVID19 management while appearing to downplay the extent of the health crisis. In what follows, I examine this misleading narrative of progress that has become an effective public relations strategy employed by Ghana’s government.

Kojo Oppong-Nkrumah. Minster of Information, Ghana (Image Credit: Reuters)
We recorded our first cases on March 12, 2020, but the government propaganda machine had already kicked in long before that. President Nana Akufo-Addo, in a well-covered media event, toured the Kotoka International Airport, the Tema General Hospital and the Greater Accra Regional Hospital and claimed that he was satisfied that we were prepared to deal with COVID19. Guess what? We weren’t. Testing could only be done at the Noguchi Memorial Institute for Medical Research (NMIMR) and the Kumasi Centre for Collaborative Research (KCCR); nationwide public education by the Information services department (ISD) only started on March 26, 2020, after cases had already been reported; and there was limited personal protective equipment for medical personnel (which was a general global challenge).
Admittedly, during the initial response, between March and July, 2020, the government adopted aggressive contact tracing and NMIMR employed novel testing strategies (using pooled testing which allowed multiple samples grouped together to be tested and if a positive confirmed, samples individually tested; and collecting sputum samples, the method used for tuberculosis sample collection, to limit the need for nasopharyngeal swabs which were in short supply). We were also the first country in Africa to institute a lockdown in March 28, 2020, lasting for 3 weeks. As these impressive responses drew international praise, government officials reminded us that we had one of the highest rates of testing in Africa.
By the time the lockdown was lifted, we had recorded more than 1000 confirmed cases and uncontrolled community spread had taken root. Then, on July 21, 2020, the government announced that they were only going to test symptomatic persons and their contacts because the backlog of samples had become unmanageable. This decision drastically reduced our testing rates (some estimate it dropped by 66% between May and August; we were testing more people at the Kotoka International Airport than the entire country combined), subsequently dropping our confirmed case count. The government then used the reduced case count to push a misleading narrative of progress and to justify further easing of restrictions. For instance, resuming sporting events (mainly football matches) and returning trotros (minibuses used for public transportation) to full capacity.
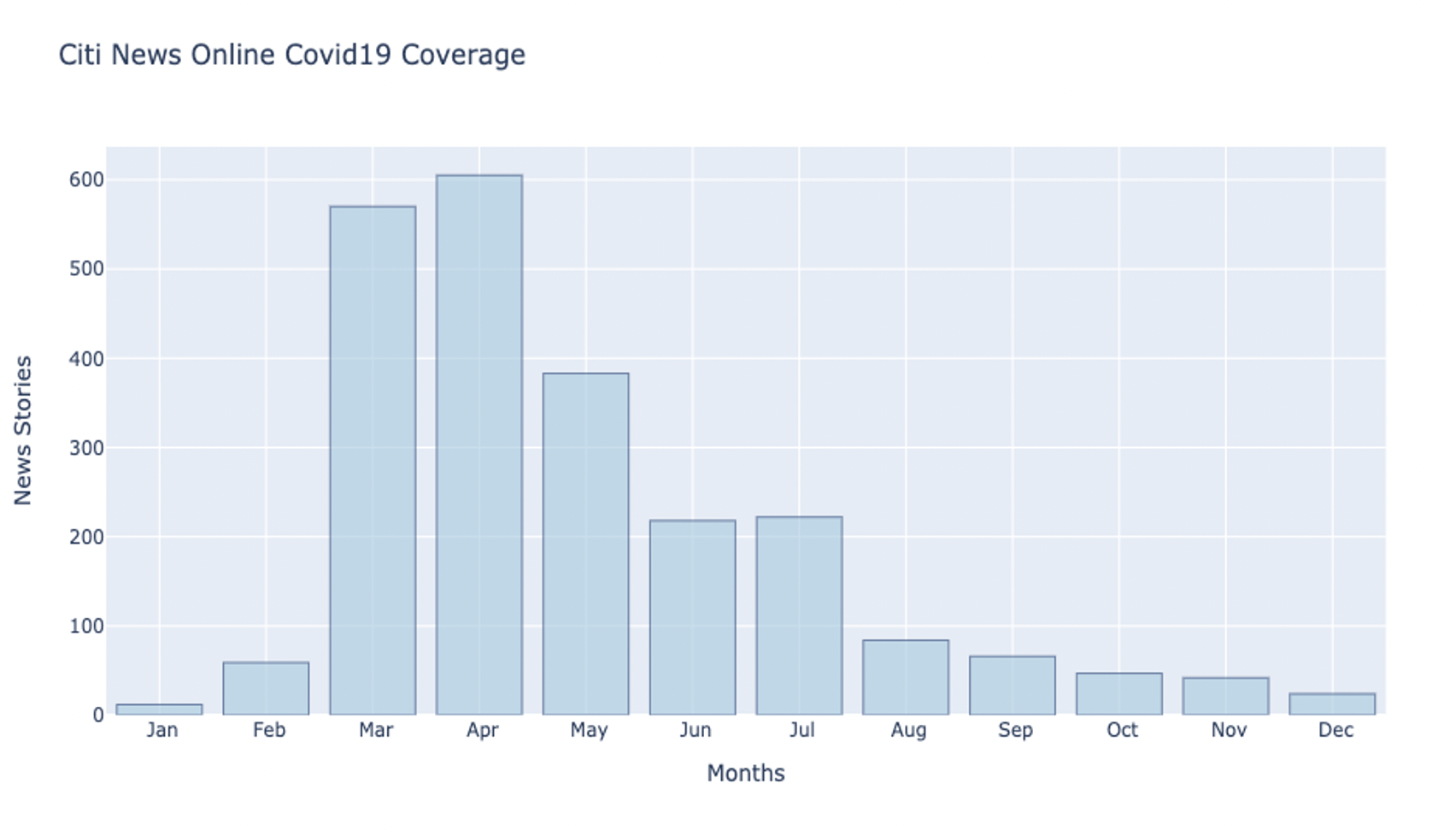
Figure 1: Search of news stories about COVID19 in Ghana on Citi Newsroom (citinewsroom.com)
This flawed narrative of progress had a negative cascading effect: media attention shifted away from the ongoing health crisis (see Fig 1 showing a steady decline in the number of COVID-19 news stories featured on Citi Newsroom Online); risk perception became so distorted that some people actually believed the pandemic was over— clubs, pubs and others were filled with people who were lulled into a false sense of security. Caution was further thrown to the wind, and as the election season ramped up, politicians organized massive rallies and parties across the country. These rallies, which the two major political parties organized, with their presidential candidates in attendance, comprised thousands of people packed together with very little physical distancing and mask wearing. At the same time, the regular press briefings and the presidential addresses on COVID19 reduced and became irregular. In March and April the president addressed the nation 4 times each month; then in July, August, September and October, just once each. The longest stretch of time between Presidential COVID19 briefings was 42 days, between November 8, 2020, and December 20, 2020.
Together with the misleading narrative of progress, another tactic employed by the government was to constantly shift our attention, and jump from statistic to statistic, selectively focusing on one category after the other and quickly de-emphasizing them as soon as they looked bad. For instance, there was first an emphasis on the number of tests conducted and then our low mortality. Then they told us to ignore the cumulative confirmed cases and to instead focus on active cases. Subsequently, they redesigned the information graphics to emphasize active cases and reduced the font size for confirmed cases (see Figure 2). Note that by this time, the criteria for discharging had also changed— rather than 3 negative COVID19 tests it became 10 days after positive test for asymptomatic patients and “10 days after symptom onset, plus at least 3 additional days without symptoms (including without fever [2] and without respiratory symptoms). [3]” This meant that people who previously would have been considered an active case would be counted as a discharged.

Figure 2 Screenshots of information graphics on COVID19 updates June 28, 2020 (left) and December 27, 2020 (right)
One powerful propaganda strategy was simply not to collect data in the first place. For instance, spin-doctor and Minster of Information, Kojo Oppong-Nkrumah, defended the recklessness of mass political gatherings, suggesting that the existing evidence did not support claims that they contributed to an increase in infections. Yet, the government did not appear to be actively screening crowds to determine how they contributed to infections. On January 31, 2021, on Joy News, after a massive spike in cases, Dr. Patrick Aboagye, Director of Ghana Health Service, also claimed that there was no evidence that crowded markets and trotros were spreading COVID19. Yet, they had previously used a market survey of adherence to masking to suggest that non-compliance was driving up infection numbers. Of course, after this comment, Prof. Awandare, Director of West African Centre for Cell Biology of Infectious Pathogens (WACCBIP), disagreed, indicating that their seroprevalence study revealed high prevalence in markets and lorry stations. Indeed, the seroprevalence study made public in early November, estimated that about 1 million people in Accra and Kasoa have been infected with COVID19 in the past. This study was largely unacknowledged and did not seem to shift the Ghana health service (GHS) COVID19 strategy. In fact, instead of acknowledging the gaps and how they would address them, GHS used the limited or non-existent data to rush to hasty conclusions in defense of reckless decisions.
Besides using information gaps to support their misleading narrative of progress, the COVID19 press briefings at the Ministry of Information became a propaganda staging ground. There was a level of performativity that served to actually do nothing, what some might call a non-performance. The press briefings became carefully choreographed encounters between officials of Ghana Health service (GHS) and the press. After GHS officials finished their presentations, Kojo Oppong-Nkrumah, the Minister of Information, would then draw attention to what reporters should focus on and how it should be interpreted. He often drew conclusions that seemed to erase the complicity of government actions and oversimplify the complexity of the data. For instance, public non-compliance to wearing masks curiously has nothing to do with poor public education and misleading low case counts. In a press briefing on November 9, 2020, Kojo Oppong-Nkrumah attempted to explain the rise in cases in October: “1st to 14th October 432 and then in the last two weeks of October, that’s where the challenge has been, 1229 new cases”, he announced. He then proceeded to show the survey of mask wearing conducted in 5 markets in the Greater Accra Region. The market survey revealed falling compliance of mask wearing and use. Oppong-Nkrumah categorically declared that “this is the data that explains why that challenge is coming up.” He used the survey to broadly argue that the lack of adherence to safety protocols had caused a “spike” in cases.
It is clear that the government could not force this highly infectious virus to play along with its propaganda. After months of inconsistent public health messaging, even with our limited COVID19 numbers, the picture remains grim. To be clear, the attempt to propagandize the pandemic may have led to more risky personal behavior. The false sense of security it created encouraged people to go out more- attending parties, in-door dinning, rallies etc. Now, more severely ill people are filling up the hospitals as the mortalities continue to increase (this has partly been attributed to the presence of the new strain first discovered in the UK). It didn’t have to be this way; honest, clear and consistent communication about the extent of spread may have helped people accurately assess their risks. This would have likely led to changes in health behavior, since the messaging would have communicated the threat of the virus and how restricting movements may limit one's exposure to the virus.

Author: Nii Kotei Nikoi
Nii Kotei studies African popular culture. He is interested in how meaning-making practices inherently relate to broader questions of power among axes of social difference and hierarchy (race, ethnicity, class, gender, sexuality, nationality and language). His research is theoretically informed by critical cultural studies, cultural production, political economy of communication, and decoloniality. He employs qualitative and visual methodologies to examine these concerns. His creative practice draws on my background in graphic design and documentary photography. Currently, his research examines development discourse in Ghanaian popular culture.